
Whether it maybe walking on uneven pavements, playing dynamic sports or landing on someone else’s foot, we may have experienced what is known as an ankle sprain. Ankle sprain are a common reoccurring injury.
How these injuries generally play out involves stepping badly or landing on an uneven surface, causing us to place pressure on the lateral rim of our foot. This is called inversion.
“Inversion-type, lateral ligament injuries represent approximately 85% of all ankle sprains.”
Conversely, if the opposite were to happen, and we tilt the ankle so that the ankle were to land on the medial rim, this is called an eversion ankle sprain. For the rest of this ankle, we will be largely talking about inversion ankle sprains, however often the case, they are treated similarly.

What is it?
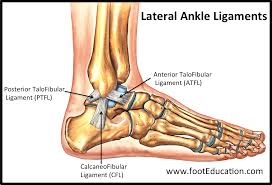
There are 3 crucial ligaments on the lateral border of our ankles. The Anterior talofibular ligament is one of them. These three ligaments connect and stabilise the ankle head (malleolus) onto the midfoot bony complex (talus). However upon extreme inversion, these ligaments may be damaged depending on the magnitude of the ankle sprain. The ligament is stretched and elongated. Repetitively spraining your ankles will also lead to ligament laxity which means that ligament integrity is lost and you’re perpetually at a higher risk of re-spraining your ankle.
There are 3 grades of ankle sprains:
Grade I involves microscopic tearing and elongating of specific proteins within the ligament. Bruising and mild swelling is present
Grade II is a moderate sprain with gross swelling and bruising. Potential looseness of the ankle joint.
Grade III is a complete rupture of the ligament, involving significant bruising and swelling. This is accompanied with ankle instability
Here now are all the questions that may be meaningful to you:
- How long will this take to get better?
- This depends on the grade of the ankle sprain. A grade 1 ankle sprain may generally heal within 4 – 6 weeks, a grade 2 may heal largely within 6 – 8 weeks and a grade 3 full rupture tear may take as little as 6 weeks increasing to 1 year. However it is just as difficult to calculate the prognosis accurately as we all have our respective confounders which may elongate how long it takes to get better (i.e eagerness to gym or play sport, not being able to dedicate enough time to recovery, not wearing protective garments, etc).
- How do I facilitate recovery? What do I need to do?
- Rehabilitation can easily be compartmentalised into 3 things:
- For grade 1 and 2 lateral ligament complex sprain – There is emphasis on early mobilisation, tentative weight bearing and guided conservative balance and strength exercises
- Certain grade 2’s and grade 3 tears may warrant immobilisation of the ankle for an extended period of days (as short as 1 week up to 6 weeks) in a cam walker (walking/moon boot) followed by proprioceptive and strength training
- Finally certain ankle sprains may require an x ray and orthopaedic intervention.
- Rehabilitation can easily be compartmentalised into 3 things:
- Will I get better?
- When it comes to functional assessment, there is good chance that your ankle will be strengthened back to baseline. However, with every repetitive ankle sprain, or even your first ankle sprain, your ligament will lengthen and make it more susceptible to future ankle sprains.
Clinical Presentation
- Inversion mechanism of injury
- Delicate weight bearing on the injured leg
- Seldom neurological symptoms – numbness, red hot shooting or stabbing pain and lancinating pain (is indicative of: paraesthesia, suspect neurovascular compromise of peroneal nerve, dermatomal involvement)
- Tenderness, swelling and bruising
- Positive special tests indicative of ligament damage
Risk Factors
- Overweight
- Foot dominance
- Flat footedness
- Inherently weak foot intrinsics and stabiliser muscles. Tightness of adjacent muscles may exacerbate the magnitude of injury.
- Previously sprained ankles – ligament laxity
- shoe type
- fatigue, competition duration and intensity of activity.
Solution
Seldom do ankle ligament injuries require surgical intervention. There are cases where surgery is not indicated even with a complete rupture or avulsion, however appropriate immobilisation is required.
Within the acute phase of ankle sprain, it is important to rest, ice, elevate and add compression within the first week. Physiotherapists will ensure that the ankle is protected while the inflammatory process continues. It is also important to adequately meet the needs of adjacent muscles with relative stretching and strengthening while the ankle is healing. As Nonsteroidal anti-inflammatory drugs (NSAIDs) may increased risk of bleeding early and the impediment of tissue healing, it is better to use natural therapies such as ice in this period. However past the first week (or 1.5 week), it may be used more prevalently.
When appropriate, ankle strengthening, range of motion and flexibility will be slowly regained. This requires a careful progression of exercise. It is important to find the balance between underdoing and overdoing exercise while healing. Doing too much exercise will cause more pain and elongate the inflammatory process, while a paucity of exercise will lead to fibrotic changes making it harder to regain range of motion.
Finally therapists will help guide you back to meaningful tasks and sports. It is important that therapists help the patient get to a level stronger than pre-injury. This is to compensate for the newly stretched ligament.
A simple ankle management program may be found here (for a grade 1 or 2 sprain) :
Week 1 – 2:
- Rest Ice Compression Elevation
- Gentile temperature regulated range of motion (as tolerated) – advocate pain free stretching while avoiding further tissue injury
- Camboot if required
- Low grade exercises: Calf raises in sitting, ankle circles, isometric eversion and inversion
- Normalise painful gait compensations
Week 2 – 4:
- Early exercises – Theraband ankle inversion/ eversion exercises, standing calf raises 3 x 15
- Moderate exercises – Squats and lunges when tolerates 3 x 15
- Balance exercises – bosu ball walking (dome side) 1 x 5 mins , single leg deadlift 3 x 3, practice low grade jogging when tolerable
- The goal is to be pain free while walking and mobilising on unstable surfaces
Week 4 – 6
- Combining strength and balance – bosu ball squats 3 x 10
- dynamic exercises – skater jumps + other variants of such
- Return to sport exercises – dynamic stepping/ change of direction
- Maintenance exercises for other muscle groups – glutes, quads, hamstrings for a safer return to sport
- At 6 weeks we would aim that the affected ankle is at 80% strength compared with contralateral lower limb
Week 6 – 8
- Full sport specific training
The common ankle sprain should not be underestimated, as one simple ankle sprain predisposes to a lifetime of reoccurring injury. Therefore it is important that rehab is actively sought to continue strengthening the ankle. This sets us up prophylactically.
Article by Joshua Shum (Physiotherapist)