
Femoroacetabular Impingement (FAI)
Hip pain may be attributable to a wide variety of causes. Femoroacetabular Impingement (FAI) is one of them. In short FAI is the growth of abnormal anatomy at the hip leading to abnormal and painful loading of the hip joint. This may further present and transform into cartilage labral injuries, bone bruising and arthritic changes as a result of abnormal articulating surfaces. FAI’s are incredibly hard to diagnose and according to Clohisy et al., the average delay to definitive diagnosis from the onset of symptoms in FAI patients is approximately 3 years.
How FAI works.
Imagine a ball and socket joint. The ball may spin, rotate and be orientated in a multitude of various degrees. This is our hip joint.
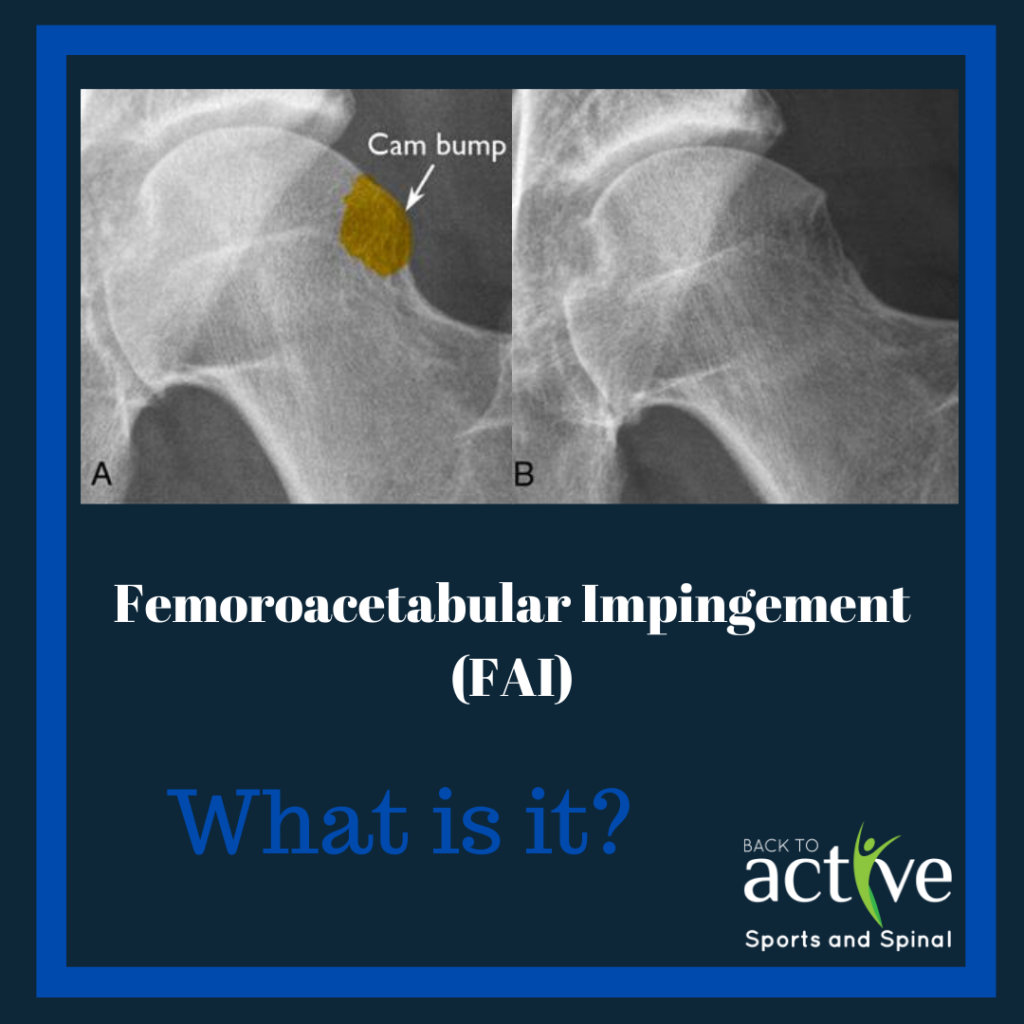
The two most common morphology abnormalities are the cam and pincer impingement.
The cam morphology describes a flattening or convexity of the femoral head neck junction while the pincer morphology describes “overcoverage” of the femoral head by the acetabulum. Either morphologies can lead to impingement symptoms.
What we need to be cognizant about is the presence of FAI morphologies without the presence of pain. The isolated presence of either cam or pincer morphology is insufficient for a diagnosis of FAI syndrome. This is because 30% of the population may have asymmetrical and asymptomatic morphologies. Therefore, there must be a coupling of FAI presentation as well as a conglomerate of signs and symptoms.
The etiology of FAI may be multifactorial. Associated developmental factors include:
- Intrinsic factors and gender
- High repetitive stress – squatting, jumping running
- Childhood developmental hip disease
- Poor union and joining of previous hip fractures
- Surgical over correction.
For most patients with FAI, the onset of FAI is quite insidious. Pain is most commonly located in the groin. However, discomfort may also be experienced in the lateral hip, thigh, low back and buttock area. FAI will be most painful with acceleration sports as well as squatting, climbing stairs and prolonged sitting. Finally, people may also complain of stiffness, restricted ROM, clicking, catching, locking or giving way of the hip.
If a FAI is suspected there should be a trial for conservative intervention. This includes:
- Activity modification – avoidance of hip deep flexion, adduction and internal rotation
- Physical therapy – manual therapy and mobility exercises
- Use of non-steroidal anti-inflammatory medications
Surgical treatment is also a viable intervention with conservative management fails. Current surgical options include arthroscopy, open surgery with surgical hip dislocation, or a combination of the two. Arthroscopy is certainly a common procedure as surgeons have access to trimming and reshaping the hip socket. Labral repair and debridement may also be performed to the surgeon’s clinical judgement. However, still note that even with conservative and potentially surgical intervention in place, some patients may not recover back to baseline.
If a FAI is suspected by you it is important that professional advice is sought immediately. This is an injury that has the potential to streamline into further damage. Therefore, it is important that conservative management may be trialled and if warranted, surgical intervention be considered.
Written by Joshua Shum Physiotherapist